I have waded into the deep waters of AI with a new chatbot. By uploading dozens of papers, presentations, and other documents that I have created over the past 10 years, I hope this Chatbot can provide lots of helpful information about cardiac disease.
Please try it and let me know if you have any suggestions.
Low Density Lipid (LDL) Cholesterol is the main cause of atherosclerosis, which is the abnormal deposition of cholesterol in the arterial wall. Atherosclerosis is the basis of cardiovascular disease.
What is a normal LDL cholesterol for a human?
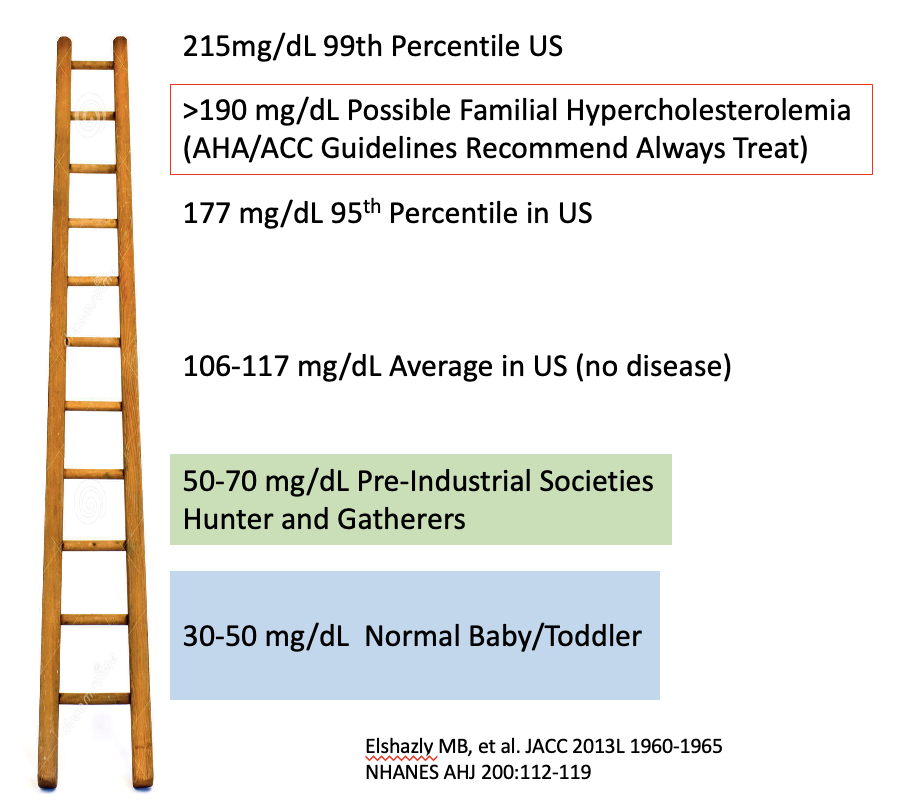
This is a an interesting question and we can look at a few pieces of evidence that support the LDL should be very low (<70 mg/dL). For example, when babies are born, the LDL is between 30-50 mg/dL. This remains true up until ~3 years of age. After the LDL does rise. There are theories that increased dietary sugar intake increase PCKSk9 expression in the liver, which in turns decreases LDL receptors. Less LDL receptors causes less LDL particles to be removed from the blood stream.
Total cholesterol is low in pre-industrial societies such as Hazda and Inuit. These societies still practice a Hunter-Gatherer lifestyle. Although they do eat animal proteins (especially the Inuit), the diet does not contain processed foods. These diets have significantly more fiber intake. People in these societies can lives in their 70-80’s without evidence of atherosclerosis.
One amazing study of the Tsimane, a Bolivan tribe, found 5x lower rates of coronary artery disease than the US population. These research scanned 705 people with a CT scanner to determine coronary artery calcifications. 85% of the study group had Zero Calcium! Of note, the average LDL of the Tsimane was 91 mg/dl.
And when you compare total cholesterol among humans versus primates and mammals, you see that there is a large difference.
O’Keefe J et al. JACC 2004:2142-2146
So we can conceptualize LDL levels on a ladder. Higher on the ladder, higher the risk of cardiovascular disease. The average LDL cholesterol in the US population on 106-117 mg/dL which is about 40-60% higher than a hunter gatherer society.
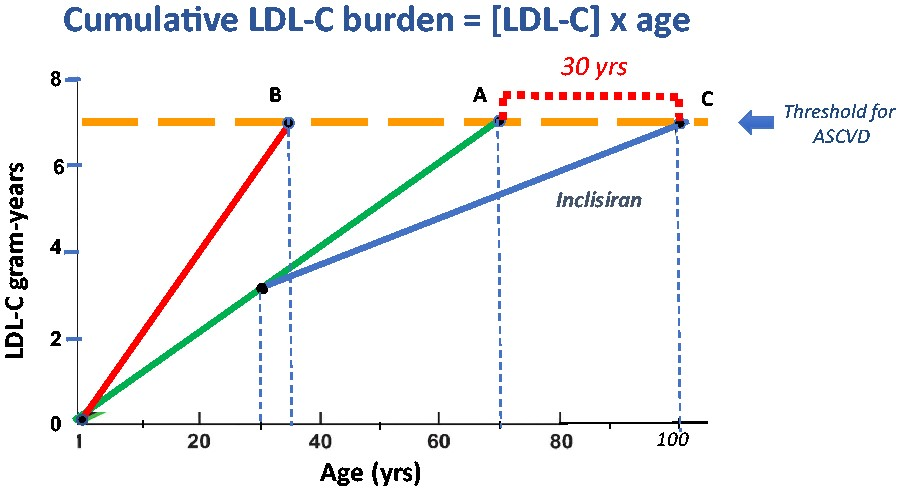
Therefore to consistently prevent atherosclerosis, maintaining a low LDL cholesterol is a key strategy. This is why Dr. Baunwald has suggested using yearly shots of incliseran to prevent cardiovascular disease. Similar to categorizing the severity of a smoker’s history in pack-years, Dr. Braunwald suggests we view cholesterol-years as an expression of cholesterol burden. The yellow line represents the cumulative exposure of a LDL 7 gm for 70 years. If we can reduce the LDL cholesterol early in life, we can delay the onset of atherosclerotic disease for 30 years.
Braunwald E. Eur Heart J 2022
I don’t think society or the healthcare system is ready to give every adult a yearly shot of incliseran. But we can all take steps to improve our diet to lower the LDL as much as possible. I suggest a Mediterranean style diet which is low in process foods and high in fiber.
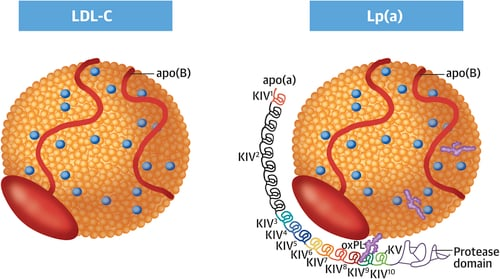
Lipoprotein A also called “LP little a”, is a known marker for cardiovascular disease. Patients with high Lp(a) levels are at increased risk (up to 4x) from stroke or heart attack. Lp(a) levels are genetically determined and don’t significantly fluctuate with dietary/lifestyle changes. About 20% of the population has elevated levels of Lp(a). Compared to other forms of cholesterol such as LDL cholesterol, Lp(a) is linked to increased inflammation, atherosclerosis, and arterial thrombosis.
While LP(a) is clearly linked to increased to cardiovascular disease, it is still unclear if it is directly causal or just a marker for disease. It is not yet established whether reducing Lp(a) actually prevents future cardiovascular disease. Currently there is no FDA approved therapy for elevated Lp(a). PCSK9 inhibitors can reduce Lp(a) levels, but it is still unclear if this effect is strong enough to reduce disease apart from the cholesterol reduction (note: PCSK9 inhibitors are not FDA approved to lower Lp(a)).
In patients with elevated LP(a), it should be considered a risk enhancing factor for future atherosclerotic disease and may help shift patient-physician risk discussions toward favoring initiation of statin therapy. Current paradigms for treatment of elevated Lp(a) suggest aggressive risk factor modification. While it has been postulated the aspirin may be beneficial in a primary prevention setting, there is no clear consensus on routine use of aspirin in this setting. There is a genetic subtype of Lp(a) carries (rs-3798220-C) which may benefit from aspirin use.
There are several ongoing trials to determine if directly treating LP(a) levels will reduce cardiovascular disease. One trial sponsored by Novartis is called HORIZONS and another from Amgen is called OCEAN.
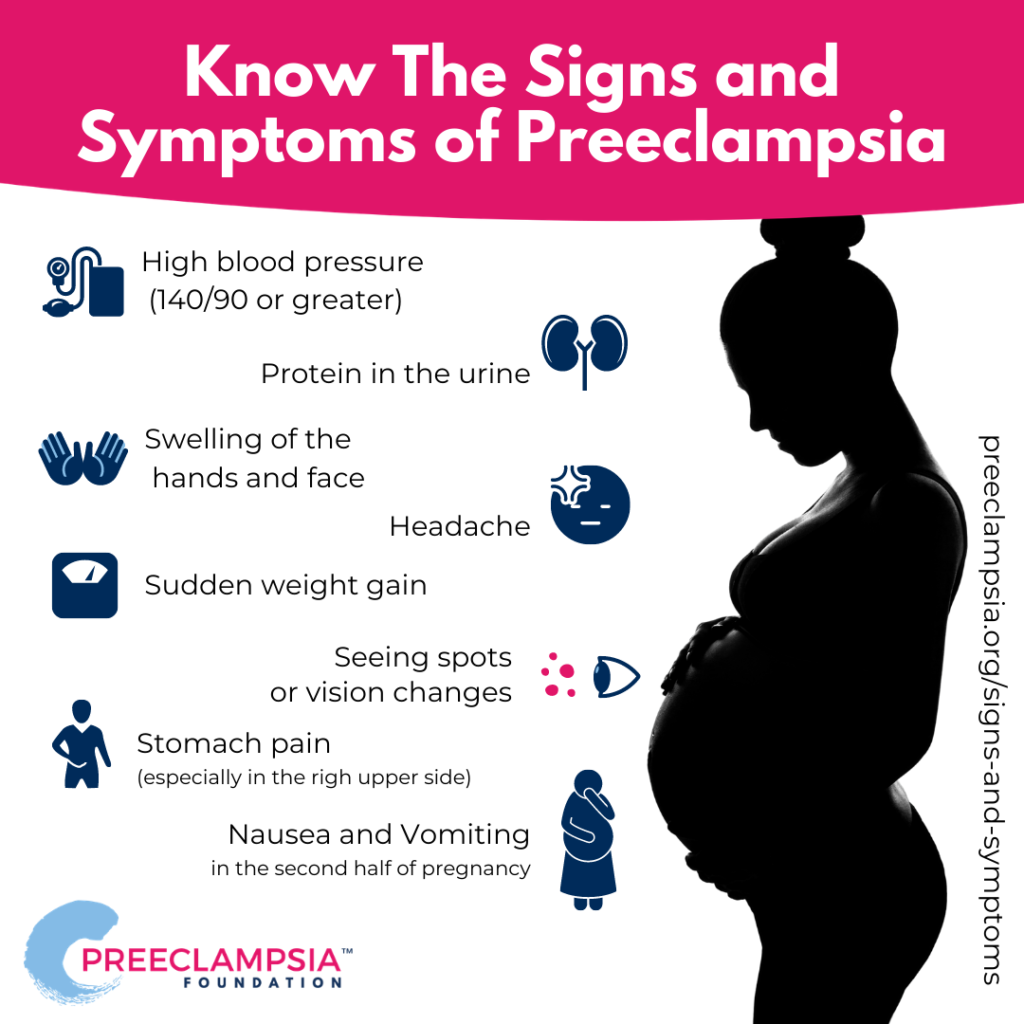
It is now more appreciated that women who suffer pre-eclampsia have long-term increase risk of cardiovascular diseases. Therefore these women need to be aware of this life-long increased risk.
Women who had pre-eclampsia should be evaluated at least once in cardiology clinic to review there current risk factors for cardiovascular disease. Education about how to mitigate the risk of heart disease should emphasize a healthy lifestyle.
Disease
Long-Term Risk
Hypertension
3.74x
Type 2 Diabetes
2.28x
Kidney Disease
3.35x
High Cholesterol
2.5x
Adverse cardiac outcome
2.0x
Please be mindful of your risks and ensure:
Eat healthy diet high in fiber and fresh veggies/fruit
Avoid high salty foods
Maintain normal body weight (BMI <25)
Exercise 3-4x a week
Monitor Blood Pressure and treat if home BP >130/85
Check cholesterol (LDL) every year
Consider obtain a coronary artery calcium score at age 50
A significant percentage of patients after COVID-19 infection will have cardiac symptoms of tachycardia, palpitations, and chest pain.
The American College of Cardiology (ACC) has published an expert consensus document to provide an overall framework for the diagnosis and management of patients afflicted with persistent symptoms followed COVID19 infection: https://www.jacc.org/doi/10.1016/j.jacc.2022.02.003
The ACC terms persistent symptoms more than 4 weeks after COVID19 infection as post-acute sequelae of SARS-CoV-2 (PASC). PASC is a constellation of symptoms which can be non-specific. In my practice, I have seen dozens of patients with symptoms such as fatigue, exercise intolerance, orthostasis, shortness of breath, and palpitations after COVID19 infection. I have also seen a few patients with these symptoms after COVID19 vaccination.
A typical cardiology workup would include: 12 lead ECG, echocardiogram, and possibly ambulatory cardiac event monitoring (i.e. Holter). Referral to pulmonology may also be needed for pulmonary function testing (PFT).
I have treated a few patients with midodrine +/- fludrocortinsone to reduce orthostatic intolerance or POTS-like symptoms.
Unfortunately there is no clear and effective treatment. Hopefully the tincture of time will resolve the symptoms.
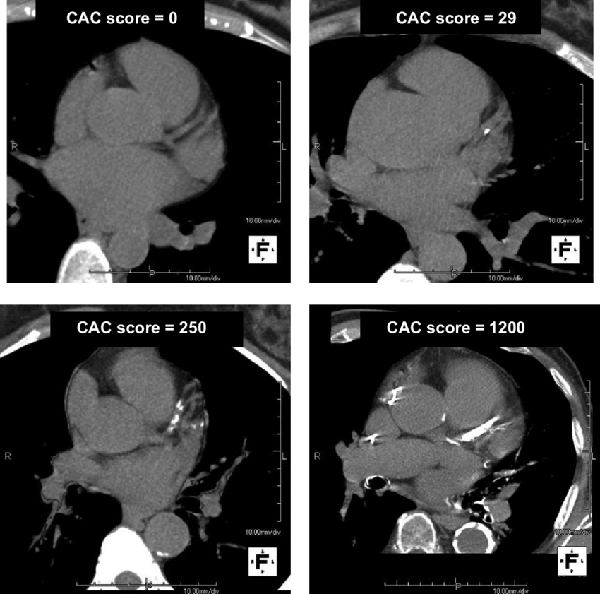
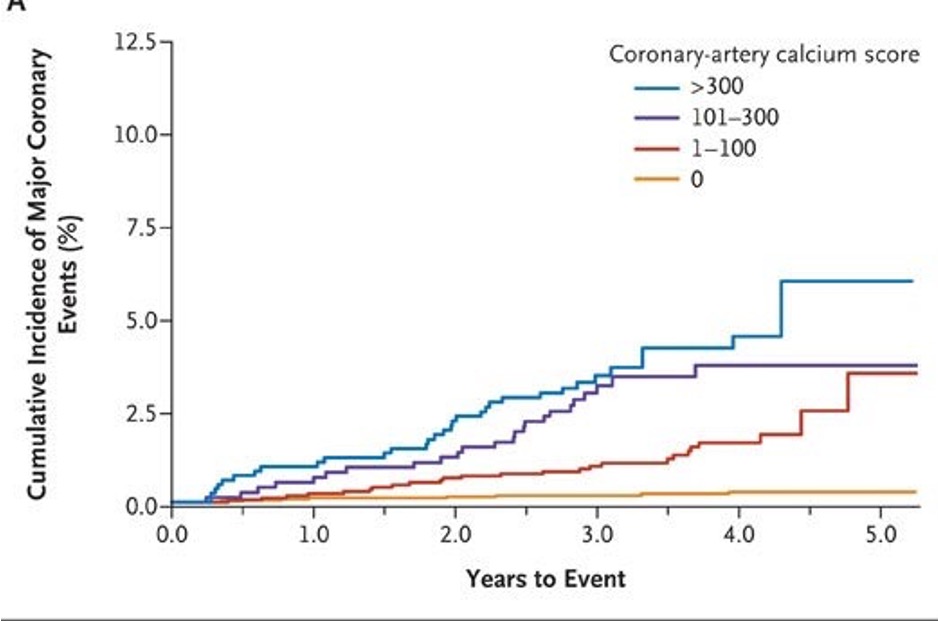
Coronary artery calcium (CAC) score has emerged as an accurate and simple method to screen for atherosclerosis and cardiovascular disease risk. The amount of calcium in the arteries correlates with overall plaque burden and greatly enhances the ability to predict risk of heart attack and cardiovascular death.
Case Studies:
Two male patients with family history of coronary disease. Neither has angina with exercise. Both would have low calculated risk by the usual ACC risk calculator. Although the younger patients has additional risk factors for CVD (fatty liver, cigar smoking), he is fortunate to have no CAC.
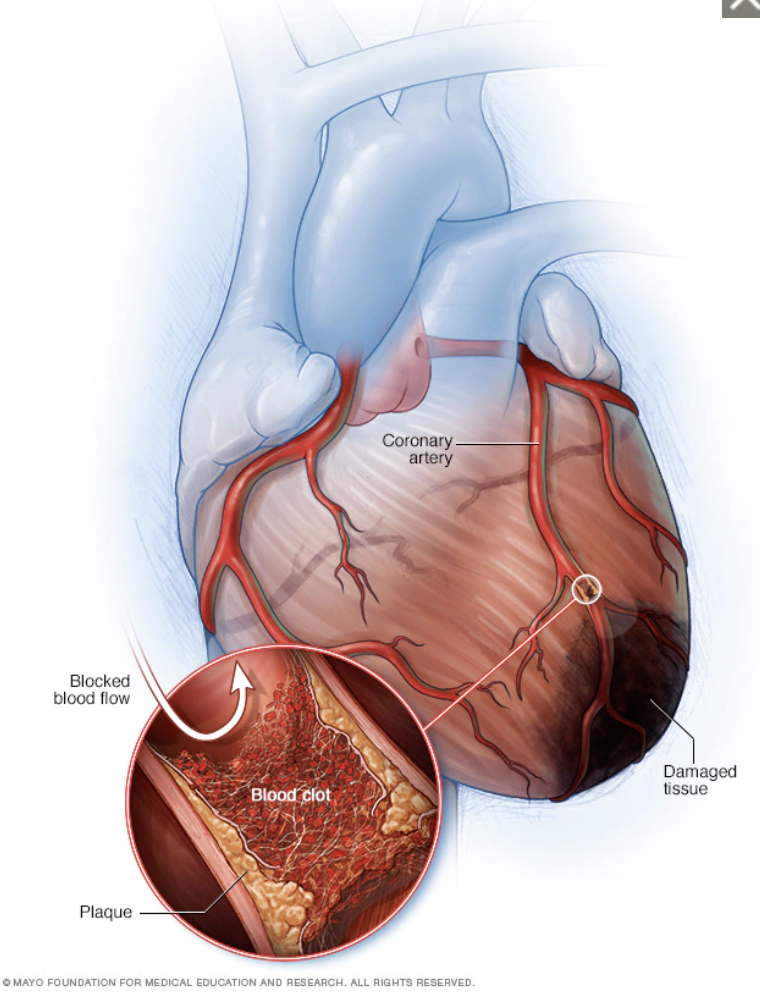
Heart Attack is a sudden blockage of blood flow due to a blood clot forming on a ruptured coronary plaqueDetrano R, et al. NEJM 2008
Most American’s eat more sodium than is necessary. Many studies have shown that excess sodium intake can increase blood pressure (hypertension) which over many years increases the risk for heart attack, stroke, and heart failure.
A single teaspoon of table salt contains >2300 mg of sodium.
Can reducing sodium intake reduce heart disease?
A few trials such as the DASH-sodium diet have shown significant reductions in blood pressure in subjects who limited sodium intake to less than 2,4000 mg.
Are salt substitutes a good option? Salt substitutes often mix potassium chloride with regular table salt (sodium chloride). Excessive potassium intake in patients with impaired kidney function could be dangerous…
Recommendations
Based on the 2013 ACC/AHA Guidelines, people with hypertension or at right for hypertension are recommended to eat less than 2,400mg of sodium a day. Furthermore, people who can reduce sodium to less than 1,5000 mg/day can expect further reductions in blood pressure and cardiovascular risk.
For the most part, foods naturally do not have much sodium. So if you can eat fresh foods, you will easily avoid eating too much sodium. Processed and manufactured foods often have sodium added to improve flavor and mask the taste of the canning process. Here’s a list some common foods and it’s sodium content: